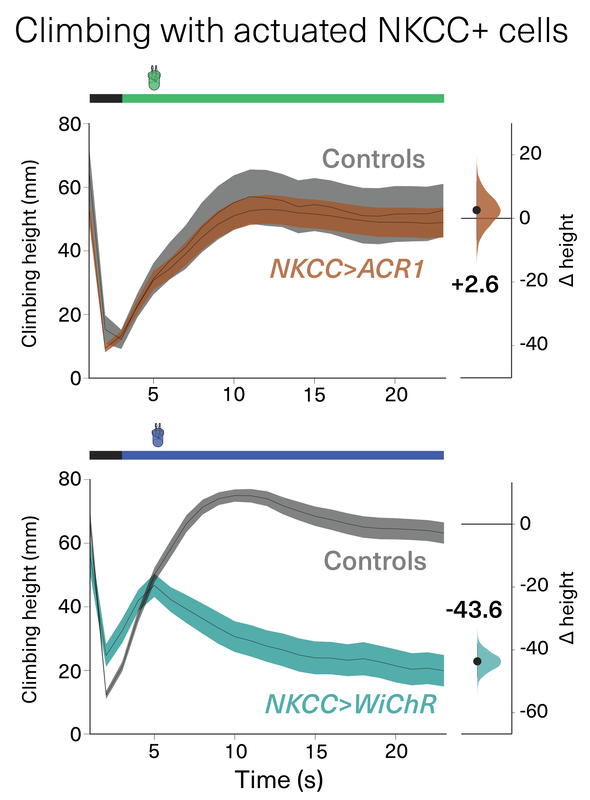
The Claridge-Chang lab evaluated the utility of the new kalium channelrhodopsins to suppress behavior and inhibit neural activity in Drosophila, C. elegans, and zebrafish. In direct comparisons with ACR1, a variety of KCRs with enhanced plasma-membrane trafficking displayed excellent potency, and with improved properties that include reduced toxicity and superior efficacy in putative high-chloride cells.
This comparative analysis of behavioral inhibition between chloride- and potassium-selective silencing tools establishes KCRs as next-generation optogenetic inhibitors for in vivo circuit analysis in behaving animals.
Read more here.
This comparative analysis of behavioral inhibition between chloride- and potassium-selective silencing tools establishes KCRs as next-generation optogenetic inhibitors for in vivo circuit analysis in behaving animals.
Read more here.
 RSS Feed
RSS Feed